Left Atrial Roof Line Ablation

Pin On Cardiology

Figure 1 Roles Of The Left Atrial Roof And Pulmonary Veins In The Anatomic Substrate For Persistent Atrial Fibrillation And Ablation In A Canine Model Jacc Journal Of The American

Left Atrial Linear Ablation Targeting The Roof And The Left Isthmus Download Scientific Diagram

Atrial Tachycardias After Atrial Fibrillation Ablation How To Manage Aer Journal

A New Approach For Catheter Ablation Of Atrial Fibrillation Mapping Of The Electrophysiologic Substrate Jacc Journal Of The American College Of Cardiology

A Navx Computer Map Of The Left Atrium A Showing A Roof Line Download Scientific Diagram

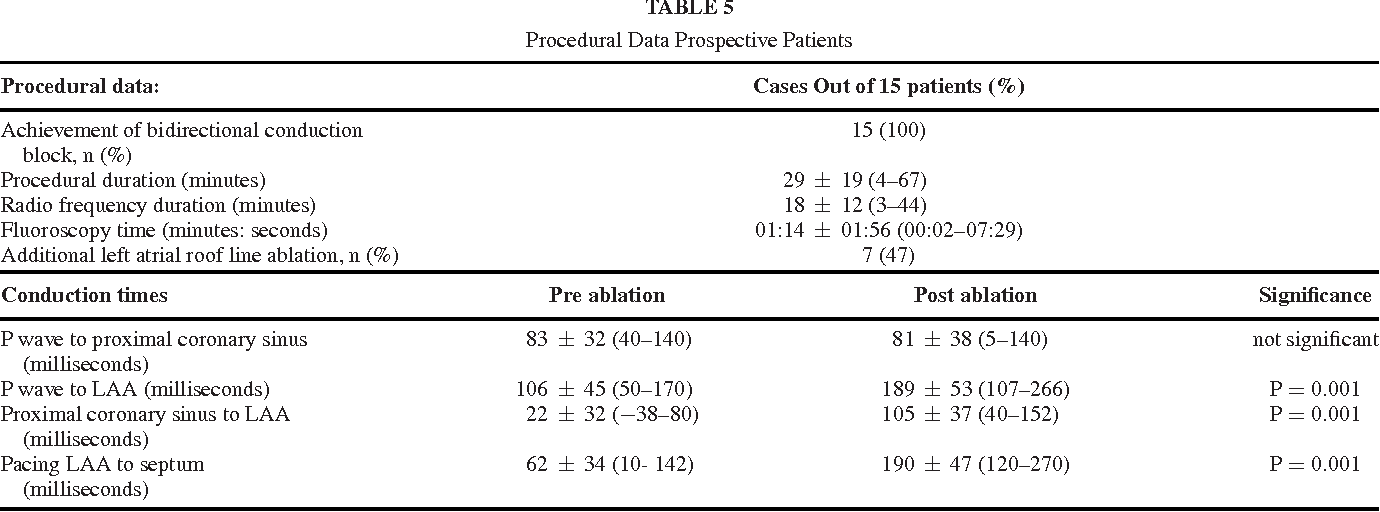
Of the several proposed linear lesions only mitral isthmus and roof line ablation remain commonly performed as an adjunct to pulmonary vein isolation in the treatment of atrial fibrillation 2 3.
Left atrial roof line ablation.

Pin On Chairs

D Po01 187 Unidirectional Block Does Not Exist After Radiofrequency Line Creation Data From Ultra High Density Mapping The Uniblock Study Id 133 Heart Rhythm Society 2020 41st Annual Scientific Sessions

A Lattice Tip Temperature Controlled Radiofrequency Ablation Catheter For Wide Thermal Lesions First In Human Experience With Atrial Fibrillation Sciencedirect
Http Onlinelibrary Wiley Com Doi 10 1111 Jocs 12092 Pdf

Scheme Of Entrainment For Patients Undergoing Ablation For Symptomatic Download Scientific Diagram

Focal Source And Trigger Mapping In Atrial Fibrillation Randomized Controlled Trial Evaluating A Novel Adjunctive Ablation Strategy Heart Rhythm

A Streamlined Approach To Catheter Ablation For Atrial Fibrillation Ep Lab Digest
Https Www Aats Org Aatsimis Sitedownloads Stars17 Saturday 1500 Saliba Pdf

Cryoballoon Ablation Of Atrial Fibrillation Using A Novel Fluoroscopy Based Anatomic Positioning System Early Experience Ep Lab Digest

Figure 2 From Efficacy Of Left Atrial Voltage Based Catheter Ablation Of Persistent Atrial Fibrillation Semantic Scholar
Https Www Ahajournals Org Doi Pdf 10 1161 Circep 117 005948

Ablation Of Long Standing Persistent Af During The Covid 19 Pandemic Ep Lab Digest
Https Www Ahajournals Org Doi Pdf 10 1161 Circulationaha 105 541052

Atrial Tachycardias After Surgical Atrial Fibrillation Ablation Clinical Characteristics Electrophysiological Mechanisms And Ablation Outcomes From A Large Multicenter Study Sciencedirect

Pdf The Relationship Of Early Recurrence Of Atrial Fibrillation And The 3 Month Integrity Of The Ablation Lesion Set
Https Www Ingentaconnect Com Content Wk Hco 2018 00000033 00000001 Art00008 Crawler True Mimetype Application Pdf

Recurrence Of Atrial Arrhythmias Despite Persistent Pulmonary Vein Isolation After Catheter Ablation For Atrial Fibrillation A Case Series Sciencedirect
Https Www Heartrhythmcasereports Com Article S2214 0271 18 30340 3 Pdf
Http Electrophysiology Onlinejacc Org Content Jcep 2 6 723 Full Pdf

Characterization Of Complex Atrial Tachycardia In Patients With Previous Atrial Interventions Using High Resolution Mapping Sciencedirect
Https Academic Oup Com Europace Article Pdf 20 Fi 3 F401 26947475 Eux350 Pdf
Http Electrophysiology Onlinejacc Org Content Jcep 2 1 27 Full Pdf
Https Academic Oup Com Europace Article Pdf 22 Supplement 1 Euaa162 347 33547648 Euaa162 347 Pdf

Atrial Flutter Thoracic Key

Atrial Fibrillation Ablation Jacc Journal Of The American College Of Cardiology

Novel Electrocardiographic Criteria For Real Time Assessment Of Anterior Mitral Line Block Jacc Clinical Electrophysiology

Non Pulmonary Vein Triggers In Nonparoxysmal Atrial Fibrillation Implications Of Pathophysiology For Catheter Ablation Della Rocca Journal Of Cardiovascular Electrophysiology Wiley Online Library

Direct Or Coincidental Elimination Of Stable Rotors Or Focal Sources May Explain Successful Atrial Fibrillation Ablation Jacc Journal Of The American College Of Cardiology
Left Atrial Appendage Conduction Jump For Real Time Evaluation Of Conduction Block Over The Anterior Mitral Annulus Line Semantic Scholar
Http Www Rhythmcongress Com Wp Content Uploads 2019 10 Pre8 Chu Antony Pdf
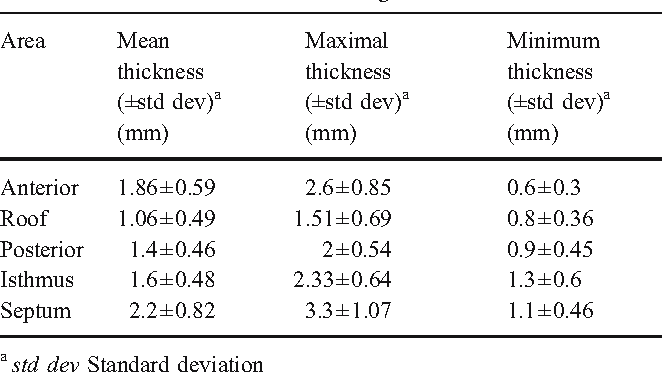
Variation In Left Atrial Transmural Wall Thickness At Sites Commonly Targeted For Ablation Of Atrial Fibrillation Semantic Scholar
Https Electrophysiology Onlinejacc Org Content Jcep Early 2017 09 22 J Jacep 2017 07 018 Full Text Pdf
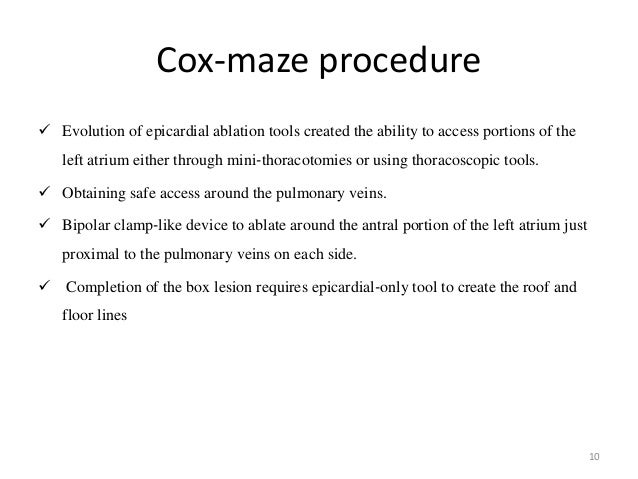
Hybrid Atrial Fibrillation Ablation

Validation Of The Noncontact Mapping System In The Left Atrium During Permanent Atrial Fibrillation And Sinus Rhythm Jacc Journal Of The American College Of Cardiology

Repeat Procedures After Hybrid Thoracoscopic Ablation In The Setting Of Longstanding Persistent Atrial Fibrillation Electrophysiological Findings And 2 Year Clinical Outcome Velagic 2016 Journal Of Cardiovascular Electrophysiology Wiley Online
Https Electrophysiology Onlinejacc Org Content Early 2018 04 25 J Jacep 2018 03 007 Full Text Pdf

Left Atrial Appendage Laa Electrical Isolation By Maze Like Catheter Substrate Modification In Presence Of Laa Occluder Device A Case Report Zanchi Clinical Case Reports Wiley Online Library

Abstract 12079 Genetic Susceptibility To Atrial Fibrillation Is Associated With Left Atrial Electrical Remodeling And Adverse Post Ablation Outcome Circulation

D Po01 150 Focal Pulsed Field Ablation For Linear Atrial Lesions A Preclinical Feasibility Assessment Id 115 Heart Rhythm Society 2020 41st Annual Scientific Sessions
Characteristics Of The Conduction Of The Left Atrium In Atrial Fibrillation Using Non Contact Mapping Sciencedirect
Https Academic Oup Com Europace Article Pdf 19 Suppl 3 Iii295 17903626 Eux158 085 Pdf
Https Www Ahajournals Org Doi Pdf 10 1161 Circep 111 970293
Http Www Internationaljournalofcardiology Com Article S0167 5273 16 33338 1 Pdf
Source : pinterest.com
